50Y/M WITH DKA SECONDARY TO SEPSIS WITH AKI
CASE:
A 50 year old male patient farmer by occupation, presented to causality with chief complaints of fever since 2 days, delayed response to verbal commands since morning and involuntary movements of left upper limb for 10-15 mins in the morning.
History of presenting illness:
Patient was apparently asymptomatic 10 days back when he had 1 episode of high grade fever, with reduced appetite, not associated with vomiting, loose stools, cough, headache, treated outside with IV fluids, ceftriaxone (2 doses) for 1 day. The patient continued to have reduced appetite, consumed only milk and liquids and continued to take OHA everyday. No reoccurrence of fever.
This morning the patient had an episode of left upper limb involuntary movements, large amplitude, low frequency? Chorea for 10-15 mins. When his GRBS was checked by RMP, found to be high and insulin given.
Patient was brought to our hospital in drowsy but arousable with painful stimuli state.
Past history:
K/C/O DM-II since 10 years on OHA
H/O RTA 4 years back, underwent nephrectomy.
H/O left sided tingling and numbness 6 months back, with no weakness and started on Tab. Clopidogrel 75mg/OD + Atorvas 20mg
Personal history:
Consumes mixed diet
Reduced appetite
Bowels regular
Micturition normal
Addictions: none
Family history:
Not significant
General examination:
Patient is drowsy but arousable with painful stimuli
Vitals:
Temp: afebrile
PR: 52 bpm
BP: 140/90 mmHg
RR: 31 cpm
Systemic examination:
CVS: s1 s2 heard
RS: BAE+ NVBS+
P/A: Soft, non tender, no organomegaly
CNS: NFND
Provisional diagnosis:
?DKA
With H/O nephrectomy 4 years back post rta
With K/C/O DM-II since 10 years









ECG:

Chest X-ray:



Treatment given:
Day-1
- NBM till further orders
- Foley’s catheterisation
- Head end elevation 30 degrees
- Inj. HAI 6IU/IV/STAT
- Inj. HAI 40IU in 39ml NS @ 6ml/hr
- Inj. Sodium bicarbonate 100mEq/IV/STAT
- IVF-0.9% NaCl (1-3hrs-10-20ml/kg/hr). Consider 0.9% NaCl for 1st 4 hrs
- GRBS hourly
- If GRBS<250mg/dl change fluids to IVF- fusodex (5% dextrose+0.45% NS) @ 150-250 ml/hr
- Next 6 hrs and 12 hrs- 0.45% NS @250-500ml/hr
- Serum K to be monitored 4th hourly
- ABG 6th hourly
- Strict I/O charting
- BP/PR/Temp charting hourly
- Inj. Piptaz 405gm/IV/STAT f/b inj. Piptaz 2025gm/IV/STAT
- Syrup ascoril/PO/TID
Day-2
Delirium secondary to uremic encephalopathy or metabolic (hyperglycaemia)
Diagnosis: DKA secondary to sepsis with AKS (resolving)
K/C/O type II DM
H/O nephrectomy 6 years back post RTA
? CVA
GRBS: 150 mg/dl
I/O: 2000/800 ml in last 24 hrs
1. Inj. PIPTAZ 2.25 gm IV/TID
2. IVF- NS@ 100ml/hr continuous infusion
3. Strict I/O charting
4. BP/PR/Temp/ SpO2 charting
5. Inj. PAN 40 mg IV/OD
6. Inj. OPTINEURON 1 amp in 100 ml NS IV/OD
7. Inj. HAI 1ml+ 39ml NS IV infusion @ 3 ml/hr
8. Inj. KCl 2 amp in 0.45 % NS@ 100 ml/hr
9. GRBS monitoring
10. Inj. 5% DEXTROSE @ 75 ml/hr if GRBS< 150mg/dl
Day-3
Sensorium improved
Subjectively- drowsy but arousable
No irritability
Objectively- conscious but drowsy
Febrile- *103* F
SPO2-91% on RA
BP- 110/70
PR- 104bpm (Relative bradycardia)
CVS-S1S2
RESP- End inspiratory crepitations B\L basal areas (R>L)
CNS- no focal deficit
No meningeal signs
P/A - no tenderness
Assessment- To rule out pulmonary pathology.
Plan- Serial GRBS monitoring and titration of insulin
Urinary electrolytes to rule out ATN.
Check on Urea and creatinine level.
GRBS: 190mg/dl
1. IVF 0.45% NS @ 100ml/hr continuous
2. Inj. HAI 1ml (40 units) + 39 ml NS IV infusion @ 3ml/hr
3. Inj. 5% DEXTROSE if GRBS< 150mg/dl
4. Inj. PAn 40 mg IV/OD
5. Inj. OPTINEURON 1 amp in 1oo ml NS IV/OD
6. Inj. KCl 2 amp in 0.45 % NS@ 100 ml/hr
7. GRBS monitoring
8. Strict I/O charting
9. BP/PR/Temp/ SpO2 charting
10. Tab. RIBOFLAVIN 10mg PO/BD
11. Inj. LEVOFLOXACIN 750mg IV/BD
12. Inj. METROGYL 100ml IV/TID
13. Tab. DOLO 650 mg TID.
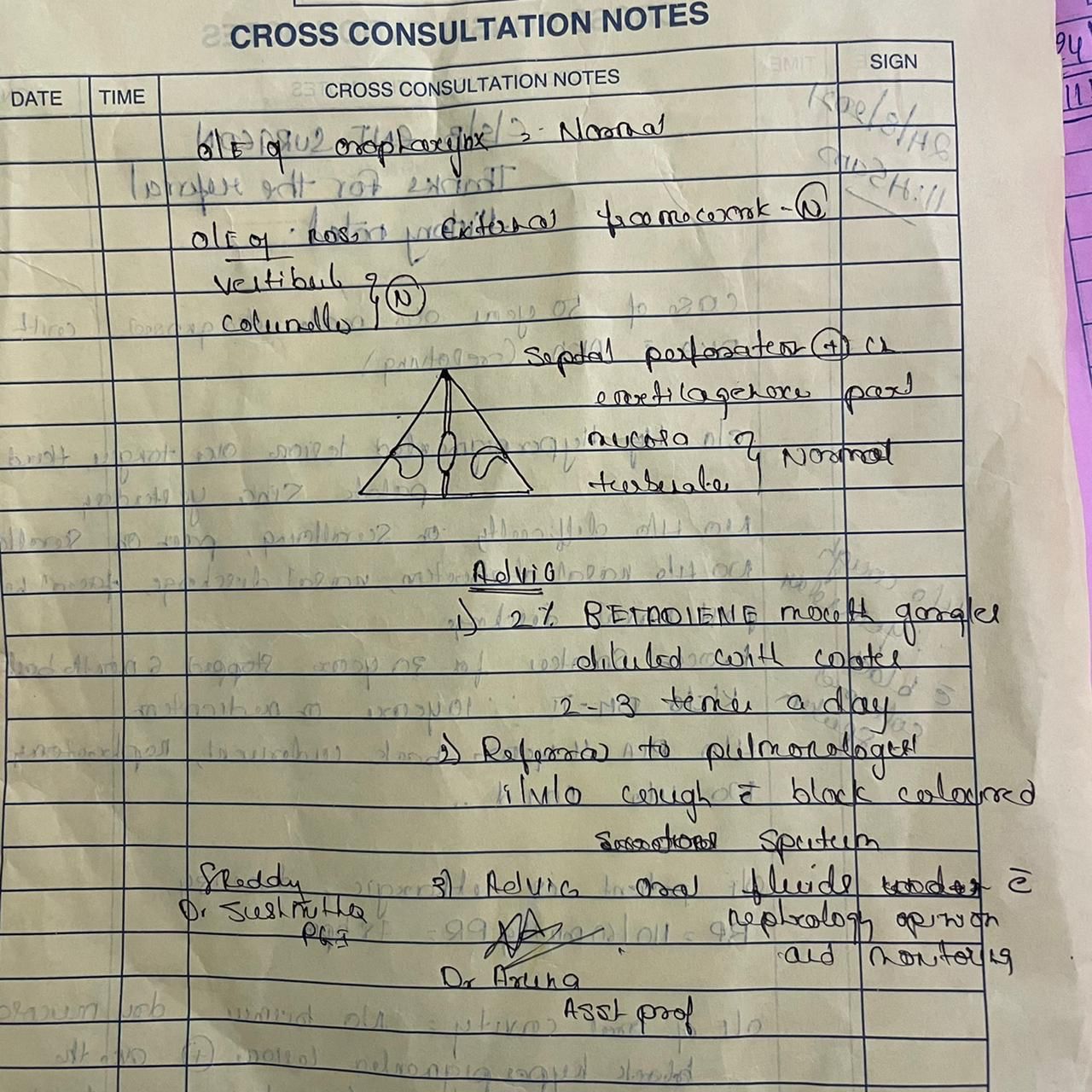
ENT referral taken for hyperpigmented lesions on the tongue and hard palate and scrapings sent for culture/sensitivity and microscopy.





1. IVF 0.45% NS @ 100ml/hr continuous
2. Inj. HAI 1ml (40 units) + 39 ml NS IV infusion @ 3ml/hr
3. Inj. 5% DEXTROSE if GRBS 150-200mg/dl
4. Inj. PAN 40 mg IV/OD
5. Inj. OPTINEURON 1 amp in 1oo ml NS IV/OD
6. Inj. KCl 2 amp in 0.45 % NS@ 100 ml/hr
7. GRBS monitoring
8. Strict I/O charting
9. BP/PR/Temp/ SpO2 charting
10. Tab. RIBOFLAVIN 10mg PO/BD
11. Inj. LEVOFLOXACIN 750mg IV/BD
12. Inj. METROGYL 100ml IV/TID
13. Tab. DOLO 650 mg TID.


Comments
Post a Comment