80 yr old acute ge secondary to aki
CASE SCENARIO
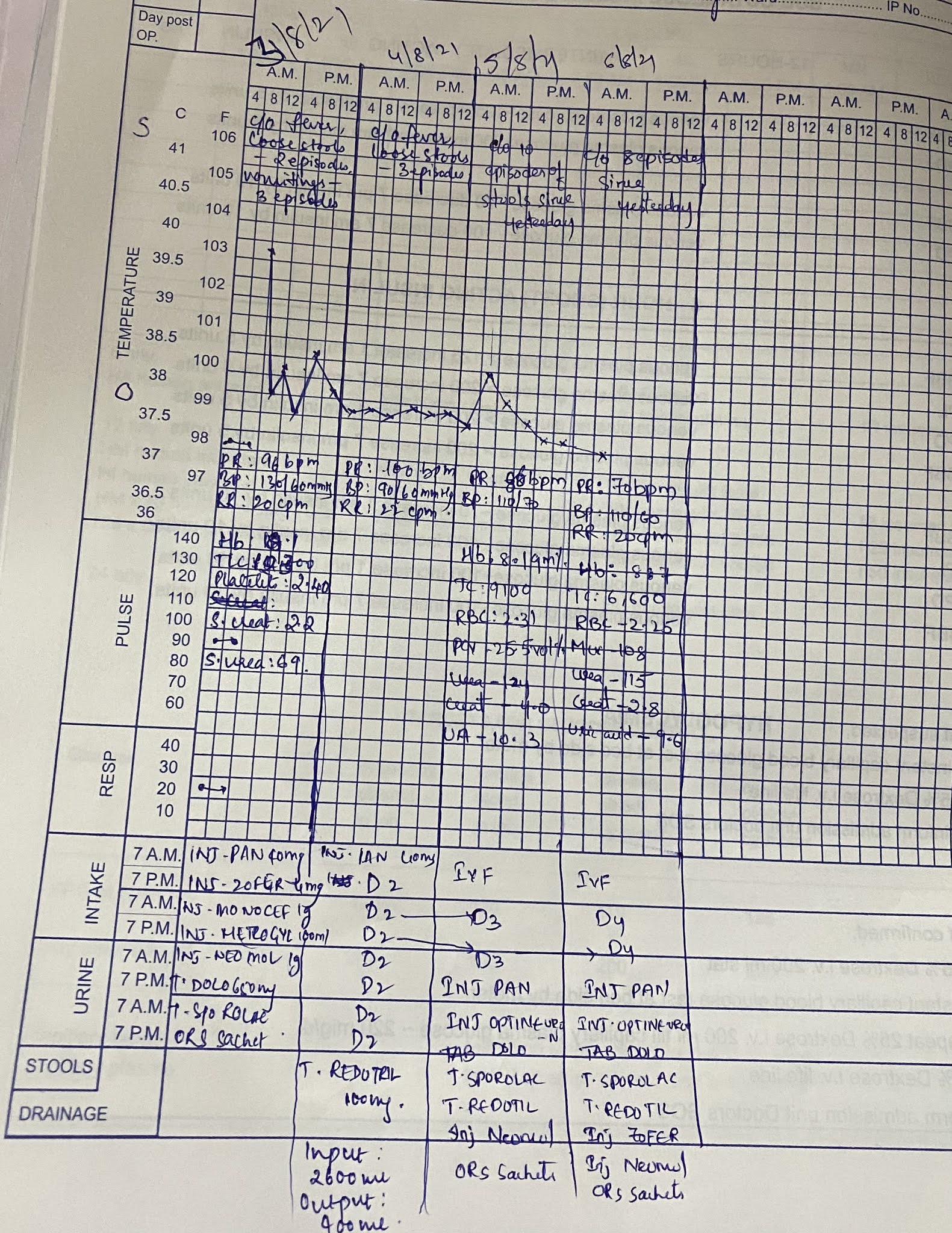
A 80 yr old female came to casuality on 03/08/2021 with cheif complaints of high grade intermittent fever, chills and rigor since yesterday, 2 episodes of loose stools since yesterday, vomitings - 3 times
HISTORY OF PRESENTING ILLNESS
The patient was asymptomatic 2 days ago after which she develop high grade intermittent fever, chills and rigor, 2 episodes of loose stooles, vomitings -3 times
No H/O of pain abdomen, cold, cough, burning Micturition and decreased urinary output
No other complaints
HISTORY OF PAST ILLNESS
Not a k/c/o DM, Asthama, Epilepsy, TB
Known case of HTN
TREATMENT HISTORY
4 yrs on tab TELMA-H 40/12.5 for hypertension
PERSONAL HISTORY
Married
Normal appetite
Non vegetarian
Mixed diet
Bowls regular
Micturition normal
No known allergies
Alcohol - occasional
FAMILY HISTORY
No H/O of similar complaints in the family
GENERAL EXAMINATIONS
No -pallor/Icterus/Cyanosis/Clubbing/Lymphadenopathy/Edema/Malnutrition
Dehydration - yes
Temperature -103 C/F
Pulse rate - 96 /min
Bp - 130/60 mm/hg
Spo2 - 96 %
GRBS - 126 mg%
SYSTEMIC EXAMINATION
CVS:
No Thrills
Cardiac Sounds - S1, S2 +
No cardiac murmurs
RESPIRATORY SYSTEM:
Dyspnoea - No
No Wheezing
Position of Trachea - Central
Vesicular sounds
ABDOMEN:
Shape - Obese
No tenderness, palpable mass, No fluid, No bruits,
Bowel sounds- present
Hernial Orifices - Normal
Liver Spleen - Not palpable
Genitals speculum examination, PV examination, P/R examination - Normal
CNS:
Level of consciousness - conscious
Speech - Normal
No signs of meningeal irritation
Cranial nerves - Normal
No motor or sensory deficit
Glassgow scale -15/15
GAIT, MUSCULO SKELETAL SYSTEM, SKIN, EXAMINATION OF BREAST, ENT, TEETH AND ORAL CAVITY, HEAD AND NECK - NORMAL
INVESTIGATIONS:





AKI 2° To Acute GE
Known case of HTN
TREATMENT
DAY- 1

Iv fluids NS, RL continues @100 ml/hr
Inj. PAN 40mg Iv/OD
1-x-x
Inj. MONOCEF 1gm Iv/BD
1-x-1
Inj. METROGYL 100 ml Iv/TID
1-1-1
Tab dolo 650 mg
Tab sporolac -DS TID
1-1-1
Inj. NEOMOL 1gm Iv/sos (if temp >101°F)
DAY-2:
Iv fluids NS, RL continues @100 ml/hr
Inj. PAN 40mg Iv/OD
1-x-x
Inj. MONOCEF 1gm Iv/BD
1-x-1
Inj. METROGYL 100 ml Iv/TID
1-1-1
Tab dolo 650 mg
Tab sporolac -DS TID
1-1-1
Inj. NEOMOL 1gm Iv/sos (if temp >101°F)
ORS sachets in 1 litre water- after each episode of loose stools
BP/PR/temp/SpO2 monitoring
Tab redotril 100 mg BD
1-x-1
DAY-3:
Iv fluids NS, RL continues @100 ml/hr
Inj. PAN 40mg Iv/OD
1-x-x
Inj. MONOCEF 1gm Iv/BD
1-x-1
Inj. METROGYL 100 ml Iv/TID
1-1-1
Tab dolo 650 mg
Tab sporolac -DS TID
1-1-1
Inj. NEOMOL 1gm Iv/sos (if temp >101°F)
ORS sachets in 1 litre water- after each episode of loose stools
BP/PR/temp/SpO2 monitoring
Tab redotril 100 mg BD
1-x-1
Iv fluids NS, RL continues @100 ml/hr
Inj. PAN 40mg Iv/OD
1-x-x
Inj. MONOCEF 1gm Iv/BD
1-x-1
Inj. METROGYL 100 ml Iv/TID
1-1-1
Tab dolo 650 mg
Tab sporolac -DS TID
1-1-1
Inj. NEOMOL 1gm Iv/sos (if temp >101°F)
ORS sachets in 1 litre water- after each episode of loose stools
BP/PR/temp/SpO2 monitoring
Tab redotril 100 mg BD
1-x-1


Comments
Post a Comment